
UNILATERAL DELAYED LEFT DEEP INFERIOR EPIGASTRIC PERFORATOR (DIEP) FLAP
Dr. Glyn Jones, MD
Plastic Surgeon, Illinois Cosmetic and Plastic Surgery, Peoria IL. Professor of Surgery, University of Illinois College of Medicine Peoria, Department of Surgery
CASE HISTORY
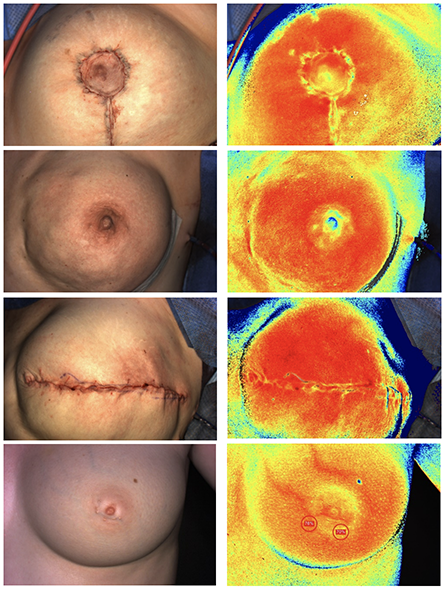
34-year old non-smoking female, BRCA1 positive, underwent bilateral prophylactic nipple sparing mastectomies with immediate direct-to-implant reconstruction. She developed an infection postoperatively that resulted in implant loss on the left side. A secondary reconstruction was performed with a DIEP flap to salvage the left breast. The flap healed well with a successful patient outcome. The perforator vessels were marked prior to surgery (Fig 1.A) based on magnetic resonance angiogram (MRA) imaging. Near infrared spectroscopy (NIRS) imaging with SnapshotNIR was used to capture a baseline tissue oxygenation image prior to elevation (Fig 1.B). The flap was harvested on two (2) perforators from the vascular pedicle. The pedicle was then anastomosed with the left internal mammary vessels.
Rapid tissue oxygenation (St O2) assessment of the wound bed and surrounding tissue.

“Knowing that the flaps are well oxygenated and viable is a key factor in guiding our decision making.”